
Recessions are easy to forecast, so how can CEOs better prepare to weather the economic storm?
‘A rising tide lifts all boats’ is an aphorism associated with the idea that good CEOs can drive business growth during the good times. However, in my experience…
exceptional CEOs drive remarkable growth during economic downturns!
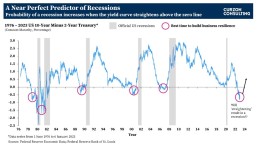
No matter what anyone tells you, recessions are easy to forecast. It’s the severity of the recession that is difficult to predict. One of the most watched charts in economics is the 10-year US treasury interest rates minus the 2-year US treasury interest rates (a.k.a. Yield Curve chart), which has a near-perfect record of forecasting recessions. The yield chart is currently flashing a ‘code red’ highlighting a recession is highly likely within the next 12-18 months. However, it is not all doom and gloom!
Smart CEOs can leverage the yield curve date to ensure their businesses are fortified to weather the upcoming economic storm. As shown on the chart, building financial and operational resistance should be a key priority of executives whilst the yield curve remains inverted!
What is yield curve inversion, and why does it matter?
To simplify… the chart shows the 10-year US treasury interest rates minus the 2-year US treasury interest rates. In a normally functioning economy, the longer the bond maturity, the higher the interest rate (yield) demanded by investors. Investors seek higher returns on longer maturing binds as risks become more difficult to anticipate the longer the term extends into the future.
However, when investors are worried about the economy, they get concerned with the ‘here and now’. Therefore, investors demand higher interest rates on short-term maturities; hence, an inversion between the 10-year and the 2-year interest rates takes place.
An inversion occurs when the 10-year US treasury interest rate minus the 2-year US treasury interest rate falls below zero.
Pre-1990s, recessions were recorded whilst the yield curves were inverted (i.e. below the zero line). Post-1990s, all recessions were recorded after the yield curves straightened (post the initial inversion).
As of 6th January 2023, the yield inverted at -0.69. This inversion is flashing a major warning signal! If history repeats again, there is likely to be a recession once the yield curve straightens again.
The question is… how deep will the recession be? That’s hard to forecast, but the current inversion rate is much deeper than what we’ve post-1990. If the inversion continues to deepen similar to the early 1980s, we could potentially see a large recession following.
So what?
As highlighted on the chart, the best time to start a business transformation programme and build financial and operational resilience is when the yield curve is inverted and well BEFORE it straightens again (i.e. rises above the zero line).
CEOs and CFOs should utilise the yield curve chart to kick start or accelerate an existing business transformation programme, well before a recession arrives.
If you are interested in learning more, please get in touch


CONTACT US TO FIND OUT HOW WE CAN HELP

Reimaging Radiology Equipment Maintenance Models - How to Enhance Cash Flow and Drive Inflation Busting Savings
With inflation at a 40-year high, how can large, multi-site operators of diagnostic equipment achieve transformative savings whilst maintaining quality?
According to Mordor Intelligence, the UK diagnostic imaging equipment market is estimated to be USD 1.1 billion in 2022 and is expected to reach USD 1.5 billion by the end of 2027.
Our research highlights, the typical profit margin on new diagnostic equipment such as a PET (Positron Emission Tomography), MRI (Magnetic Resonance Imaging), CT (Computed Tomography), Fluoroscopy, Ultrasound, X-Ray, etc... is 10-15%. However, the profit margin on maintenance contracts is > 35%.
The typical annual maintenance cost of an MRI scanner is £50,000-£70,000 and CT Scanner is £30,000-£50,000. The sum cost of all the individual maintenance contracts can mount up very quickly to several million pounds!
The actual cost of a maintenance contract can vary depending on volume discounts, hours of operation, uptime guarantees, and scope of what is included or excluded inclusions – coils, helium, etc…, along with other cost drivers.
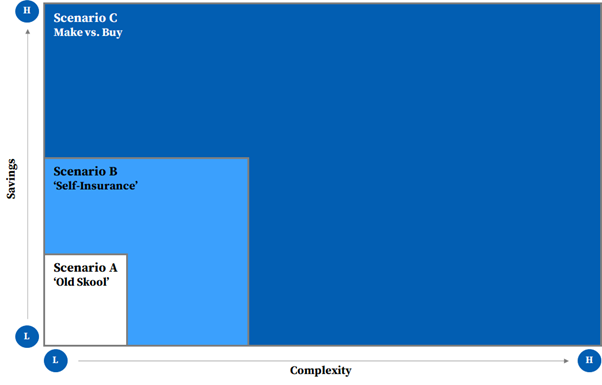
We believe there are 3 key operating models with each one driving a progressive level of savings. Scenarios B and C deliver transformative, inflation busting savings, but are the most complex to implement.
Savings vs. Complexity
Over the past few years, some organisations have turned to third-party maintenance service providers as an alternative to traditional Original Equipment Manufacturer (OEM) warranty and post-warranty support. This move has yielded substantial savings. However, that is just one solution amongst a range of others.
Scenario A – ‘Old Skool’
Under Scenario A, an organisation negotiates a full-service, gold-standard, maintenance contract with an OEM or third-party maintenance service provider.
‘Old Skool’ model can generate 10-15% savings.
Scenario A works well for a single or small hospital / diagnostic service provider business. For a large private hospital group or a diagnostic imaging service provider, this model is ‘old skool’, and worst of all, the buyer transfers significant value to the seller.
For organisations that operate a larger portfolio of diagnostic equipment, where there is a critical mass, our extensive and deep understanding of the market shows two alternative models. Both models require an open mind and can be explored together to ‘turbo-charge’ saving.
Scenario B – ‘Self-Insurance”
Under Scenario B, an organisation leverages a ‘self-insure’ model where it adoptings a risk management technique in which the company accrues a ‘pool of money’ to be used to remedy an unexpected loss from equipment breakdowns. Organisations can self-insure against equipment breakdown, and mitigate risk of large unforeseen losses by taking out implementing an excess insurance policy.
Under this scenario, an organisation buys a preventative maintenance (PM) only contract from an OEMs (Original Equipment Manufacturers) or third-party maintenance service providers, with a pre-negotiated price list for parts. The organisation pays for breakdowns as and when needed from accrued funds.
If risk is –managed appropriately, organisations can significantly enhance cash flow and savings.
‘Self-insurance’ model can generate 15-25% savings.
Scenario C – ‘Make vs. Buy’
Under Scenario C, an organisation makes a ‘make-or-buy’ decision where it chooses between setting up an in–house maintenance organisation (people, process, and systems) versus purchasing the service in part or whole from an OEM or third-party maintenance service provider.
‘Make versus buy’ model can generate 25-40% savings.
Under both Scenarios, an organisation can decide to carve-out some or all types of the diagnostic equipment for self-insurance, based on a risk assessment of service levels and uptime guarantees required per site or department.
The additional savings can be used to reinvest in new equipment, upgrades and/or drive digital transformation programmes to enhance productivity of the radiology department and improve administration, technician, clinician and patient experience.
Failure to get this right can have a material, knock-on impact on operations, patient and clinician experience, and a material loss of revenue whilst a machine is out of use.
How Can Wwe Help?
We have developed a deep understanding of the diagnostic imaging equipment market. We help clients to challenge the status quo and drive transformative benefits via the successful implementation of Scenario B and/or Scenario C.
For Scenario B – ‘Self-Insurance’, we have a methodology and proprietary analytics tools that allow us:
- accelerate the evaluation of a ‘Self-Insurance’ model
- assess financial treatment of accruals
- design options based on risk tolerance of the business
- develop a business case
- develop management information dashboard to monitor and track solution
- implement solution
For Scenario C – ‘Make vs. Buy’, we have a methodology, proprietary analytics tools and experience designing in-house operating models, that allow us:
- accelerate the evaluation of a ‘Make vs. Buy’ model
- perform maintenance demand analysis by geography
- design new Target Operation Model (TOM) options for the ‘Make’ solution
- develop a business case
- develop implementation and risk mitigation plan
- embed new TOM within an organisation
If you are interested in learning more, please contact me at chetan.trivedi@curzonconsulting.com.
CONTACT US TO FIND OUT HOW WE CAN HELP

2022 MCA Awards Winners
We are so very proud to announce #CurzonConsulting, has won the Commercial Impact #mcaawards 2022 award, with #RamsayHeathCare. Representing the very best of our consulting business, it’s such an incredible achievement to be recognised for our Procurement Transformation Programme. The judges said this was a team that: “brought specific expertise to a problem and rebuilt the procurement capability at speed, changing hearts and minds in the organisation.”
Established by the Management Consultancies Association, the representative body for the UK’s leading management consulting firms, the #MCAAwards demonstrate the transformational work the sector has undertaken during the last challenging twelve months.
The remarkable achievement marks the eight consecutive years that Curzon Consulting has been a finalist at these prestigious awards.
Commercial Impact: Procurement Transformation Programme with Ramsay Health Care UK
Ramsay Group operates a global network of 530+ healthcare facilities across 11 countries.
The pandemic exposed an over-reliance on a ‘single’ income source. With all elective activity (e.g., joint replacements, cataracts), the primary income source, halted overnight, but a high fixed cost base remained.
As a response, Ramsay UK embarked on an ambitious growth & efficiency programme. Curzon was engaged to design and deliver a Procurement Transformation programme.
Over 9 months, we took a pragmatic, agile and “together” approach to accelerate benefit delivery, particularly in high spend / high complex clinical spend categories.
By assessing the existing PO against a methodical and objective review against 8 dimensions we highlighted several data-driven insights; fundamentally, the PO only managed 44% of total spend; hence lack of PO involvement resulted in suboptimal category /supplier management and savings delivery.
Improvement opportunities were incorporated into the design of the new Procurement Organisation.
Our methodology was specifically adapted to address demand-side cost optimisation levers.
Through a deep dive into orthopaedics, a key benefit delivered in Orthopaedics came from ensuring the Surgeon selected the appropriate implant system (metal or ceramic) to match the patient’s profile (e.g., age, gender).
A well-established norm in Orthopaedics is to routinely implant, high quality, lower-cost metal vs. ceramic hip systems into >70-year-old patients. Our analysis showed Surgeons at Ramsay UK implanted costly ceramic hip systems in 33% of >70-year-old NHS patients. The NHS reimbursement for a complete hip replacement is fixed, so every incremental switch from ceramic to metal impacted the bottom line.
Surgeons had little comprehension of how their hip selection decisions impacted Ramsay UK’s profitability. Our insights directly influenced the Orthopaedic Steering Group’s new policy which required Surgeons to utilise lower-cost metal hip systems in older NHS patients.
Curzon established an open, trusted, and collaborative way of working with the Ramsay team, and by adopting a “one team” approach with the PO we ensured everyone involved with the procurement transformation owned the outcome and maximised the benefits from knowledge transfer during Wave 1.
Fundamentally a key part of the relationship was to ensure recommendations on cost improvement would not compromise clinical outcomes and patient satisfaction.
Wave 1 has delivered £multi-millions in incremental annualised savings. In addition, the savings have translated into several £100 million worth of shareholder value.
Commenting on the success – Ramsay Health’s CFO Peter Allen said:
“Curzon helped us obtain the confidence and operational ‘can-do’ to drive incremental savings sooner than we could have expected, and then to push on to best practice performance.
Their skill was in balancing pace of change and the results imperative with the need to take the organisation with them on the journey. A key achievement was building the necessary collaboration between the many functions that needed to act together to drive benefits in complex clinical spend categories.
Curzon’s strong analytical expertise, and ability help us to take a critical view on the “art of the possible” and bring the team along on the journey to demonstrate benefits delivery was a critical success factor.
The result was a tangible and ongoing commercial win, and a new Procurement Organisation to drive cost leadership, profitability and sustainability going forward”
A massive congratulations to the Curzon Consulting team and Ramsay Health Care UK and the other finalists.


CONTACT US TO FIND OUT HOW WE CAN HELP

We are delighted to welcome a new Partner for Financial Services Sector!
Curzon Consulting has appointed Andy Stewart as Partner – Financial Services, starting in October.
Andy will help drive the strategy in the financial services market, which is core to Curzon’s growth plans for the future. Working with Douglas Badham, Partner & Financial Services Sector Lead, Andy will be responsible for developing new and innovative propositions and go-to-market approaches as well as managing some of Curzon’s long-term client relationships.
Andrew Morgan, Managing Partner, Curzon said: “It’s fantastic that Andy has joined the team. He brings a wealth of background and experience that will help us add even more value to our financial services clients”
Douglas Badham, Partner & Financial Services Sector Lead, Curzon said: “I look forward to working with Andy as his expertise and strong client relationships will be invaluable to us as we execute our growth strategy”
Andy Stewart, Partner – Financial Services, Curzon said: “I’m excited to be joining the team at Curzon as they have long been committed to outstanding client service and the delivery of tangible results for their clients. I’m looking forward to getting started”

CONTACT US TO FIND OUT HOW WE CAN HELP

CIPS Awards Winners
Last night at the CIPS Excellence in Procurement Awards, we won “Best Procurement Consultancy Project of the Year” for our collaboration with Ramsay Health Care UK.
Congratulations to both teams!
Procurement Transformation Programme with Ramsay Health Care UK
As a pandemic response, Ramsay UK embarked on an ambitious growth & efficiency programme. Curzon designed and delivered a substantial cost reduction and Procurement Transformation programme.
Over 9 months, we defined a pragmatic and agile approach to implementing a best-in-class procurement organisation with an increased mandate, able to accelerate benefit delivery, and manage high spend / high complex clinical spend categories.
We helped Ramsay UK to deliver £multi-millions in incremental annualised savings. In addition, the savings have translated into several £100 million worth of shareholder value.
View the full case here – https://www.curzonconsulting.com/procurement-consultancy-project-of-the-year-ramsay-healthcare/
CONTACT US TO FIND OUT HOW WE CAN HELP
UK’s Leading Management Consultants 2022
We are delighted to have been recognised for the fifth consecutive year as one the ‘UK’s Leading Management Consultants 2022’ by the Financial Times.
Recommended across 8 categories and with our first Gold Award, the annual rating, compiled with data company Statista is based on endorsements by clients and peers and demonstrates our consistent year on year sector and service line growth.
Consulting companies are awarded Bronze (recommended), Silver (frequently recommended) or Gold (very frequently recommended).
Sectoral expertise
- Construction & Infrastructure – Gold
- Financial Services – Silver
- Public & Social Sector – Silver
- Healthcare – Bronze
Consulting services
- Digital Transformation – Silver
- Operations & Supply Chain – Silver
- Strategy – Silver
- Sustainability – Bronze
Managing Partner Andrew Morgan said
We are absolutely delighted to see the continued progression of Curzon, competing alongside some major consulting brands. I am so proud of the team, and this emphasises their commitment and dedication to deliver tangible results for our clients in a range of markets through strategic, operational and transformation delivery.
CONTACT US TO FIND OUT HOW WE CAN HELP

Hip & knee implant manufacturers – The value creation opportunity
If hip and knee implant manufacturers want to stay relevant, and “move the needle” on value creation, they need to play big or go home!
An aging (ageing) population is driving absolute sales, but over the past few years, primary hip and knee procedures have become commoditised, which has resulted in margins being squeezed for both hospital providers and implant manufacturers.
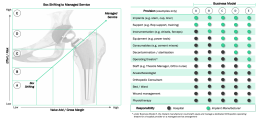
Implant manufacturers have an opportunity to transform their business model, away from traditional “box shifting” product selling (driven by monthly sales targets) to a high value add, high margin managed service proposition, where multi-year partnerships are formed with hospital providers. Implant manufacturers need to provide additional services along the value chain, especially as health systems move towards value-based care models.
The Value Creation Opportunity
About the author




CONTACT US TO FIND OUT HOW WE CAN HELP

Congratulations to Our 2021 MCA Awards finalists
We are delighted to announce that Curzon Consulting are finalists in 2 categories of the Management Consulting Awards 2021, representing the very best of our consulting business.
Established by the Management Consultancies Association, the #MCAAwards demonstrate the transformational work the sector has undertaken during the last challenging twelve months.
2021 marks the seventh consecutive year that Curzon Consulting has been finalists at the prestigious awards.
Commercial Excellence
Curzon with AIG – ‘Back to Life’ – Fast-Tracking to Leadership in Customer & Profit Retention
Read More
After a period of impressive top-line growth, AIG Life’s leadership now concentrated on driving for profitability on a US GAAP basis. Working with Curzon to isolate what could best deliver profit uplift, we zoomed in on a stubbornly un-moving customer persistency rate and recognised that every 1% point of lapse averted would yield significant and multiplicative profit gains.
Curzon was engaged on an ambitious programme to rapidly get control of lapse and release commercial benefit, and to build the capability to achieve best practice retention management. This was an enormous challenge given the starting point: no set persistency strategy, an absence of key lapse analytics, retention not owned or resourced in the organisation, and a lack of lapse prevention and turnaround processes.
Over 11 months through 2019, we took a pragmatic, agile, and ‘together’ approach to accelerate to retention excellence, securing the organisation’s buy-in to what it would take to get there, and quickly demonstrating the commercial, operational and customer benefits of joined-up retention management. Curzon enabled the new cross-functional working essential for success, and gave the business the structures and confidence to operate highly effective preventative and save processes – internally and leveraging external partners.
Among the prime watershed moments were revealing how:
- a shift in distribution mix from advised face-to-face to telesales had created a hitherto unseen problem of drop-out inside first 3 months
- customer communications from welcome onwards needed to explain clearly the personal value of life insurance, and how holding it ensures financial provision for those you love
- rather than automatically cancelling customers on request, customer service had a responsibility to engage them before they make a potentially uninformed decision
When the business took the reins 3 months after improvements were implemented, lapse rate had been reduced to the best practice % mark on a run-rate basis and incremental revenue and profit benefit unlock was exceeding our original target. This translated annualised into 5-figure policy saves and a cumulative £multi-million gain in Pre-Tax Operating Income by 2023. The business had taken ownership of a new retention management function, with a new Lapse MI suite providing the predictive insights to continually optimise retention. Beyond achieving the agreed objectives, the work also led to complementary projects including work to minimise drop-out in the Bank partnership sales channel.
Commenting on the success, AIG Life CFO Donald MacLean said:
“Curzon helped us obtain the confidence and operational ‘can-do’ to get control of lapse sooner than we could have expected, and then to push on to best practice performance.
As always, their skill was in balancing pace of change and the results imperative with the need to take the organisation with them on the journey. A key achievement was building the necessary collaboration between the many functions that needed to act together to manage retention in a joined-up way.
The result was a tangible and ongoing commercial win, and a vital new balance struck between sales and retention for business profitability and sustainability”
People
Curzon with Highways England – ‘Project Performance Accelerator – Enhancing delivery capabilities through innovative approaches and working relationships to achieve HE delivery goals
Read More
Project Performance Accelerator (PPA) was designed to develop and implement a delivery mechanism for Highways England’s (HE) overarching Business Transformation Programme, addressing inconsistent levels of capability throughout HE’s Project Management community and developing highly skilled project delivery teams. Overall, HE’s three main Major Project programmes account for 80 projects worth more than £23bn, each being delivered by a supply chain or contractor led by a Project Management team.
PPA’s leader Steph Illingworth engaged Curzon to interpret and structure her Vision of the PPA Programme into clear deliverables, shaping the fundamentals. There was consensus on cultural flaws and ineffective ways of working. Revealing a deeply siloed organisation with multiple departments or technical areas that lacked collaboration or a holistic view of the primary objectives and deliverables: projects were not executed on time and within budget, nor maximising benefits and social value. Also, capability development and training programmes were too theoretical and onerous, focusing on processes and systems rather than people, impacting the overall project success.
Focusing on performance management, capability development, project control capability and enhancing commercial acumen, the PPA Programme included two outputs as the medium for change: An Immersive Learning Experience and Digital Project Management Guidebook.
The Immersive Learning experience was designed to disrupt the way programmes are delivered. The Digital Project Management Guidebook contained PM content selected through independent reviews and capability assessments. Both outputs were crafted around the project lifecycle of typical HE infrastructure projects, set to be delivered in-person over a period of 18 months. Cohorts were selected to receive a tailored experience, improve project team maturity, and provide a solid foundation for capability uplift to achieve clear learning outcomes and benefits.
At the heart of the PPA philosophy was to enable project teams to grow, enhancing ‘ways of working’ whilst bolstering project performance. These included a “working better together model”; a fundamental shift in the way individuals interact and take ownership of overlapping project aspects and problem-solving techniques. This, along with the Immersive Learning, reinforced the Programme’s success, shifting the focus from systems and processes to people.
The pandemic introduced significant challenges, necessitating the immediate conversion of the Programme from in-person workshops to a virtual setting. The team adapted structures and materials, incorporating a variety of software suites to enhance the learner experience. Frequent interaction and close collaboration with the internal and senior stakeholders were critical to maintaining speed and delivery, adopting a fail-fast, fix fast approach to syllabus creation
The consulting team could interpret the client’s vision into a clear pathway, support and enhance the design to become one of the most successful transformation project delivered in HE.
The Digital Project Management Guidebook launched in August 2020 via four interactive webinars to c.300 employees have now received over 1,000 unique viewers. A modified deployment strategy was adopted in light of the pandemic, redesigned as a remote Immersive Learning Experience. However, over 5,049 hours of remote learning have been received by 100 staff through 9 project teams, enhancing teams’ capability with a combined portfolio value greater than £3.3bn.
Congratulations to all of the other finalists.

CONTACT US TO FIND OUT HOW WE CAN HELP

UK’s Leading Management Consultants 2021
Ranked in the Top 20 of the UK’s consulting firms, we are delighted to have been recognised for the third consecutive year as one of the ‘UK’s Leading Management Consultants 2021’ by the Financial Times.
Recommended in seven categories compiled with data company Statista, the annual rating is based on endorsements by clients and peers and demonstrates our steady consistent year on year sector & service line growth.
Consulting companies are awarded Bronze (recommended), Silver (frequently recommended) or Gold (very frequently recommended).
Sectoral expertise
- Construction & Infrastructure – Silver
- Financial Services – Bronze
- Healthcare – Bronze
- Public & Social Sector – Bronze
Consulting services
- Digital Transformation – Bronze
- Operations & Supply Chain – Bronze
- Strategy – Silver
Managing Partner Andrew Morgan said
We are thrilled to see the continued progression of the firm, competing alongside some major consulting brands. I am really proud of the team and this reinforces their dedication to deliver tangible results for our clients in a range of markets through strategic, operational and transformational delivery.
CONTACT US TO FIND OUT HOW WE CAN HELP

The accelerated adoption of drones in healthcare
We explore how the 2020 coronavirus crisis has accelerated the use of drones in the delivery of healthcare.
Drones in Healthcare
The commercial use of drones has steadily been gaining traction over the last decade.
The global market for medical drones was valued at USD $88.2 million in 2018. It is expected to witness 24.7% CAGR from 2019 to 2025. The UK market is anticipated to see even higher than 25% CAGR from 2019 to 2025. The global circumstances resulting from the coronavirus pandemic are likely to increase demand for unmanned aerial vehicles (UAVs) and drive the value of the drone market up even higher than forecast.
Drones have the potential to transform the delivery of healthcare. They have a large spectrum of medical uses that could be particularly valuable during this pandemic:
- Search and Rescue: searching vast areas for people in need of rescue/help in any environment
- Transport/Delivery: rapid delivery of medical supplies to rural areas between hospitals/labs or directly to the person in need
- Medical Care: remote delivery of medical advice/care

Despite wide potential applications in healthcare, the use of drones in practice has been fairly limited. Safety and security concerns have led to tight regulations on airspace. This makes it difficult to phase in drones for practical (rather than recreational) use. Drones have a bad reputation due to their potential abuse in breaching privacy, violating human rights and irresponsible use by hobbyists, particularly at airports. Consequently, only a small proportion of the potentially vast benefits offered by drones in healthcare have been realised.
COVID-19 impact on drones in healthcare
The coronavirus crisis has acted as a catalyst for the adoption and acceptance of drones in healthcare. There are two main reasons for this:
- The need to deliver medical care/supplies quickly is more urgent
- Social distancing and quarantine measures have made remotely operated systems particularly valuable
As a result of coronavirus, how has drone use changed or adoption accelerated? We’ve included some examples below.
Dutch company Avy manufactures wing drones for use in urban healthcare logistics, rural delivery of supplies, and first response emergency services. Avy responded to the pandemic by exploring the use of wing drones to transport COVID-19 samples from small municipalities to labs in larger cities. This would help contain the virus and minimise risk of the virus spreading.
We spoke to Patrique Zaman, Founder of Avy, about the healthcare challenges that Avy is trying to overcome.
This is an example of a drone company, Manna Aero, that changed their focus from food delivery to medicine delivery during the pandemic.
The Irish start-up launched their drone delivery service earlier this year, with the aim of moving road-based food delivery into the skies. Manna Aero’s trial delivery of takeaways to college students in mid-March had to be halted due to the coronavirus lockdown, but this did not deter them from switching focus to help in the crisis. The company has instead been working with the Irish Health Service Executive to deliver medicines and other essential supplies such as break and milk to vulnerable people in the rural town of Moneygall. Local GPs write prescriptions after a video consultation, which the drones deliver directly to homes. This represents a first in Ireland. Manna Aero is equipped to handle up to 100 deliveries a day, and hopes to bring trials to the UK soon.
The UK’s lockdown in 2020 triggered the government to grant permission for a UAV to deliver medical supplies across the Solent to a hospital on the Isle of Wight. This is part of a UK government project to develop a system allowing manned and unmanned aircraft to operate in the same airspace.
The UAV, developed by the University of Southampton and funded by the start-up Windracers, was given permission to fly as part of the British government’s Covid-19 response. It has a range of 1,000km and can carry up to 100kg.
Compared to the more traditional ferry, this novel approach allows faster, more frequent, and more reliable delivery of medical supplies.
The Covid-19 response has triggered a partnership between the drone delivery provider Skyports and Thales to trial the delivery of medical supplies.
The two-week pilot is backed by NHS Highland, and Argyll and Bute Council, with drones supplied by unmanned aircraft-maker Wingcopter. The delivery service will be based in Oban. It aims to ensure that isolated communities on the Isle of Mull (16km away) have access to COVID-19 tests and sufficient personal protective equipment (PPE).
This trial is a crucial milestone for unmanned aviation in the UK. It was granted as an exception to current rules by the Civil Aviation Authority.
Zipline is a US drone company that delivers supplies to rural communities in Rwanda and Ghana. In order to support the Covid-19 response in Africa, Zipline changed its focus to using drones to provide clinics with PPE and coronavirus test samples. The lightweight drones deliver to clinics up to 85km away. There are plans to use the drones to deliver supplies directly to the elderly and vulnerable who need to self-isolate.
Zipline CEO Keller Rinaudo thinks that drone deliveries could play a vital role both during the current crisis and in the coming months and years.
The Chinese government has been proactive in piloting ways to incorporate drones into their response to the coronavirus.
Drones originally designed to spray pesticides have been adapted to spray disinfecting chemicals in public spaces. Testing the use of drones to deliver of medical samples began in February, with over 20 flights per day at peak operation in Zhejiang Province. Consumer delivery of essential items has also been trialled, with e-commerce company JD developing a drone team to deliver to Anxin’s semi-isolated islands.
Future outlook
The unprecedented circumstances brought about by Covid-19 have kick-started the use of drones in new and exciting ways, but we are only scratching the surface of their full potential.
To progress, we need to learn from this pandemic and make changes that will ultimately lead to a better healthcare experience. Rather than relying on experimentation, we should pre-plan how drones can be used during disease outbreaks and make appropriate investments. Drones need to be integrated into planned health responses. In addition, coordination between the public and private sector will be crucial to overcome regulation by civil aviation authorities.
It is obvious that drones have a big role to play in the delivery of healthcare. The route to unlocking their true potential will offer exciting and rewarding opportunities in the future.
How Curzon can help
Curzon Consulting help with strategy and digital transformation. We have experience working in collaboration with companies to embed technology into their organisation. Curzon can:
- Conduct feasibility studies
- Build a business case and commercial offering
- Design the most appropriate operating model and integration plan
- Conduct a technical requirement assessment
Get in touch to find out how we can help or arrange a free virtual meeting with our Healthcare partner, Chetan Trivedi.
The authors

We can help you to improve patient outcomes with digital strategy, transformation and patient experience.